Scapular Variability During Shoulder Elevation
Assessing the movement capabilities of the shoulder complex in individuals experiencing pain and/or movement limitations can often seem challenging secondary to the number of muscles that influence the shoulder.
When we are met with this kind of complexity, it’s helpful to have a framework to guide our assessment process and help us gather important information that can be used to guide our treatment/rehabilitation. A framework does not have to perfectly characterise what’s happening, but it just has to provide some simplicity in the face of complexity, and this ultimately helps you become clearer when making decisions about what exercises may be most appropriate to use to drive adaptation.
When it comes to the shoulder complex, this is where it is helpful to consider the interaction between segments instead of only trying to see how muscles are lengthening/shortening, or how well each muscle is handling forces. Of course, we will be assessing both & challenging both through our exercise strategies. But, we do need to understand what kind of muscle & joint/segmental behaviour we’re going to bias as we deliver load/stress, and using segmental movement to guide that understanding can really simplify things
The two segments that we will discuss here within the context of shoulder elevation are the humerus & the scapula.
Shoulder elevation basics
The shoulder represents the interaction between multiple segments (rib cage, clavicle, scapula, humerus). When you ask someone to move their shoulder, you’re getting an insight into how these segments are interacting with each other.
When research looks at the biomechanics of shoulder elevation, they categorise elevation into three different planes
- Forward flexion (sagittal plane)
- Scaption (scapular plane)
- Abduction (frontal plane)
This is an important categorization, particularly when you are assessing the available variability at the shoulder, because the scapula & the humerus will interact in different ways during each of these elevation planes.
At IKN, a key portion of the framework we use to guide our assessment of the shoulder involves assessing the capacity of the scapula & humerus to couple appropriately during flexion versus abduction, mainly because the scapula & humerus will behave differently in these planes. We are not looking for “dysfunctions” or “impairments,” but the capacity of the segments to express certain movement behaviours.
Let’s explore this in more detail below.
Scapular & humeral coupling during flexion & abduction
When we assess movement, we use a segmental-based analysis versus a joint-based analysis. So, for us, shoulder flexion would represent humeral flexion with a certain scapular behaviour. Shoulder abduction would represent humeral abduction with a certain scapular behaviour.
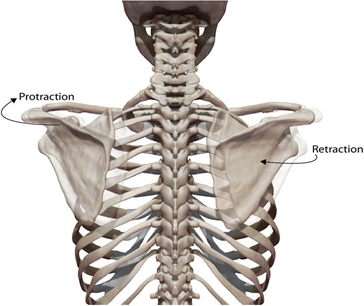
When we flex our humerus in the sagittal plane, the scapula initially needs to protract & internally rotate. This internal rotation of the scapula allows the glenoid cavity to point more into the sagittal plane to facilitate the movement of the humerus in the sagittal plane.
When we abduct our humerus, the scapula will bias a more retracted & externally rotated position. This external rotation of the scapula will point the glenoid cavity into the frontal plane more to facilitate movement of the humerus in the frontal plane.
Try this:
If you were to retract & externally rotate your scapula now, maintain that scapular position, and then try to flex your humerus (keeping it in the sagittal plane), you will likely struggle to flex the humerus beyond 90 degrees.
Similarly, if you were to protract & internally rotate your scapula now, maintain that scapular position, and then try to abduct your humerus (keeping it in the frontal plane), you will also likely struggle to abduct the humerus beyond 90 degrees.
This is the coupling behaviour we are talking about.
But, one of these planes of elevation requires more rotational variability of the scapula relative to others.
What happens towards the end-range?
As we progress beyond 90-120 degrees of flexion, the scapula will eventually externally rotate and posteriorly tilt to help flex the humerus towards end-range. What is also necessary here is appropriate coupling between the thoracic spine/rib cage & scapula to encourage this scapular external rotation. In order for the scapula to externally rotate, the thoracic spine needs to have the capacity to extend.
So, during humeral flexion, the scapula expresses more variability as it moves through internal rotation through the early/middle phases of flexion, and eventually into external rotation during the end-ranges.
During humeral abduction, the scapula maintains a scapular external rotation bias through the entire range of motion.
Why is this important?
When our goal is to restore variability to the shoulder complex, identifying the capacity of segments to move into specific directions is an important part of the process (but of course not the only part).
It’s also important to consider this within the context of the client’s aggravating movements & other subjective limitations.
Is there more of a muscular & joint limitation or a lack of tolerance (increased sensitivity/pain) when moving into flexion or abduction? Or both?
If there’s a limitation during flexion, we can consider if the scapula has the capacity to protract & internally rotate. If it can’t protract & IR, we can utilise exercises that build the scapula’s ability to protract & IR.
What if the limitation is closer towards the end-range of flexion? We can consider if the scapula has the capacity to externally rotate.
What if there’s no limitation in humeral flexion, but they’re limited during humeral abduction? Then, we can consider if the scapula has the capacity to externally rotate and choose exercises to build that capacity if necessary.
Of course, it’s not this simple. We have to integrate these movement capacities with the subjective experiences of the client.
What if you determine they lack capacity to flex the humerus and they have limited protraction. But, they have pain when you’re loading scapular protraction. How do you navigate this during the rehab process?
Learn more
These are the questions we answer and the processes we navigate during our courses. If you want to learn more, be sure to check them out! See you there!